Non-surgical. Minimally invasive. No impact on sexual function.
Prostatic artery embolisation is a non-surgical, minimally invasive, safe treatment with no impact on erection or ejaculation, and effective for treating benign prostatic hyperplasia, a very common condition that appears with age. Around 20% of men in their fifties experience symptoms related to this condition.
Minimally invasive outpatient procedure under local anaesthesia without scarring
Performed by an interventional radiologist under imaging guidance
Efficacy confirmed by numerous recent scientific studies
Covered by mandatory basic health insurance (LAMal) in Switzerland
Sexual function preserved with no impact on erection or ejaculation
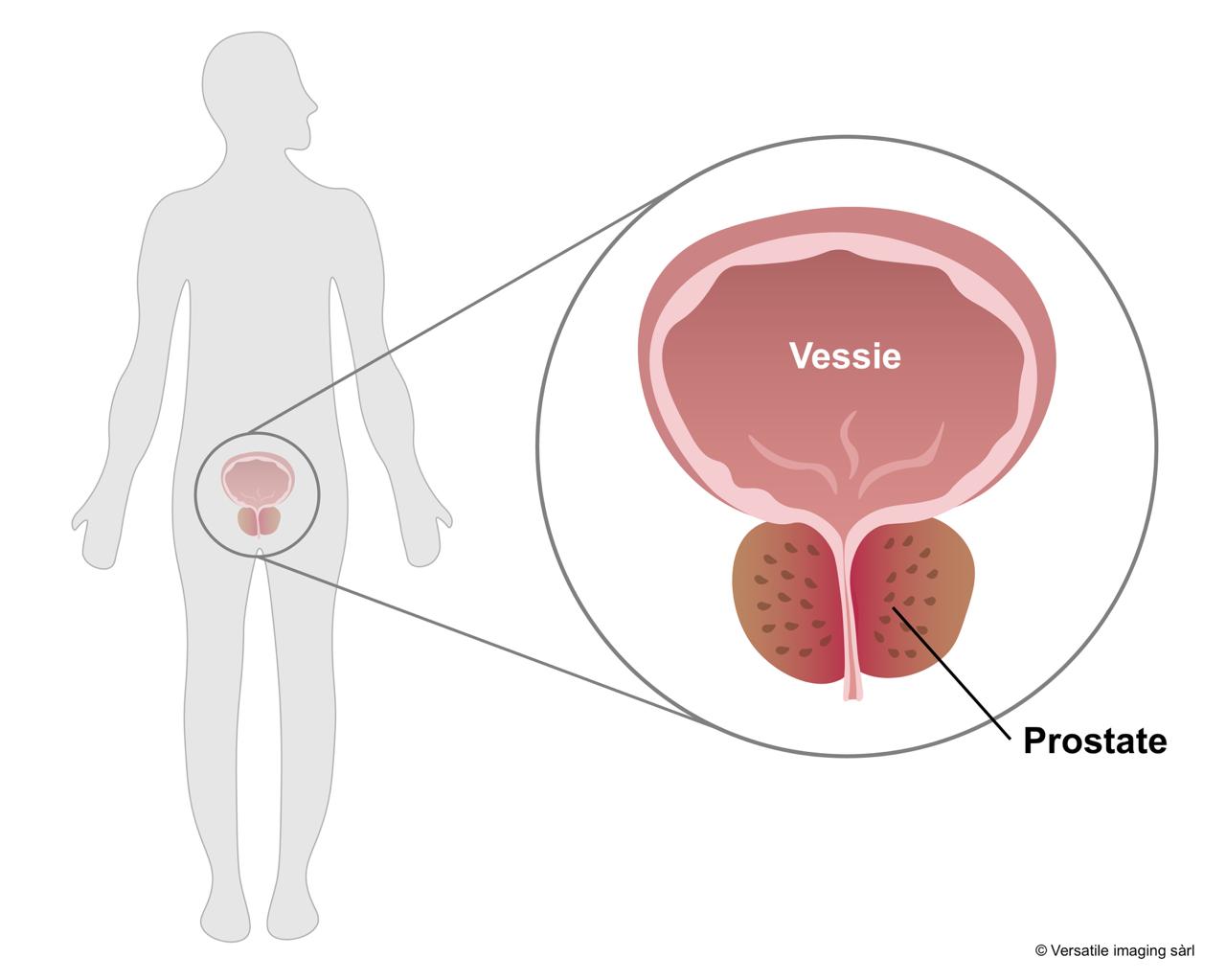
Benign prostatic hyperplasia is a common condition in our ageing society. It is estimated that 60% of men at age 60 are affected, with troublesome symptoms in 25 to 50% of cases. The prevalence increases with age, reaching 90% of men at age 90. Under the effect of hormones and with ageing, the prostate becomes hypertrophied, with the development of benign tissue called adenoma. This growth compresses the urethra, which is the channel running through the centre of the prostate for urine evacuation to the penis, creating an obstruction to urine flow.
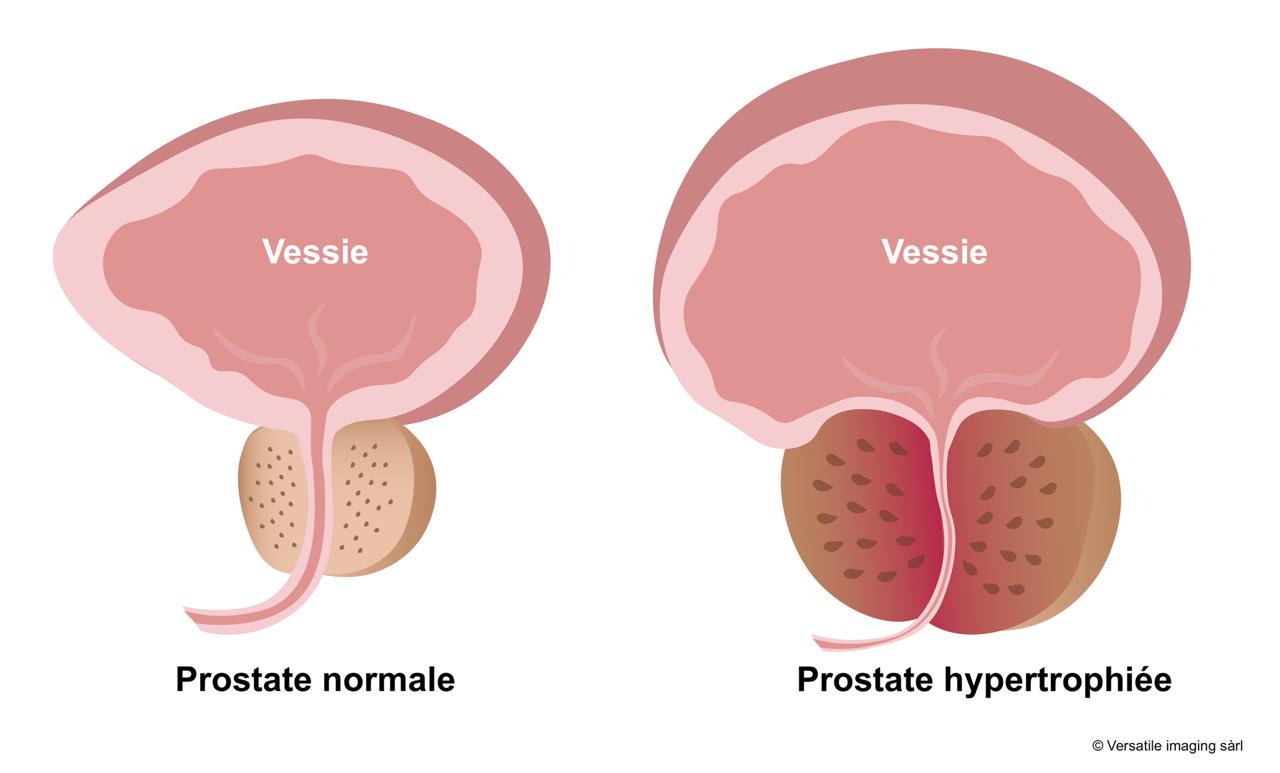
So-called "obstructive" symptoms represent difficulty emptying the bladder during urination due to blockage of the urethra.
So-called "irritative" symptoms correspond to frequent urges to urinate, night-time waking or rising, caused by bladder irritation from the enlarged prostate.
Sometimes, the patient can no longer evacuate urine at all — this is called acute urinary retention, which is treated as an emergency by inserting a bladder catheter.
This condition is not merely an inconvenience — it can lead to kidney failure if the kidneys are chronically exposed to urinary hyperpressure caused by this obstruction.
Current treatment of benign prostatic hyperplasia includes:
Pharmacological treatment is often proposed as first-line for early-stage disease. Several types of molecules can be prescribed by your urologist.
Alpha-blockers allow the smooth muscles of the prostate and bladder neck to relax, facilitating the passage of urine during urination. They are often prescribed for moderate to severe symptoms. They have moderate efficacy but often cause side effects (dizziness, fatigue, hypotension, retrograde ejaculation).
5-alpha-reductase inhibitors belong to another class of treatment. They reduce the conversion of testosterone to DHT (the activated form of testosterone) and decrease prostate volume. Their side effects (decreased libido, erectile dysfunction, gynaecomastia) are particularly dreaded by patients wishing to maintain a fulfilling intimate life.

Surgical treatment — open, laparoscopic or robotic prostate resection — is obviously the most effective treatment since the prostate is surgically removed, but it is also the most invasive, performed exclusively under general anaesthesia during hospitalisation. It is carried out by urologists. Given its heaviness, this treatment is rarely offered to treat benign prostatic hyperplasia.
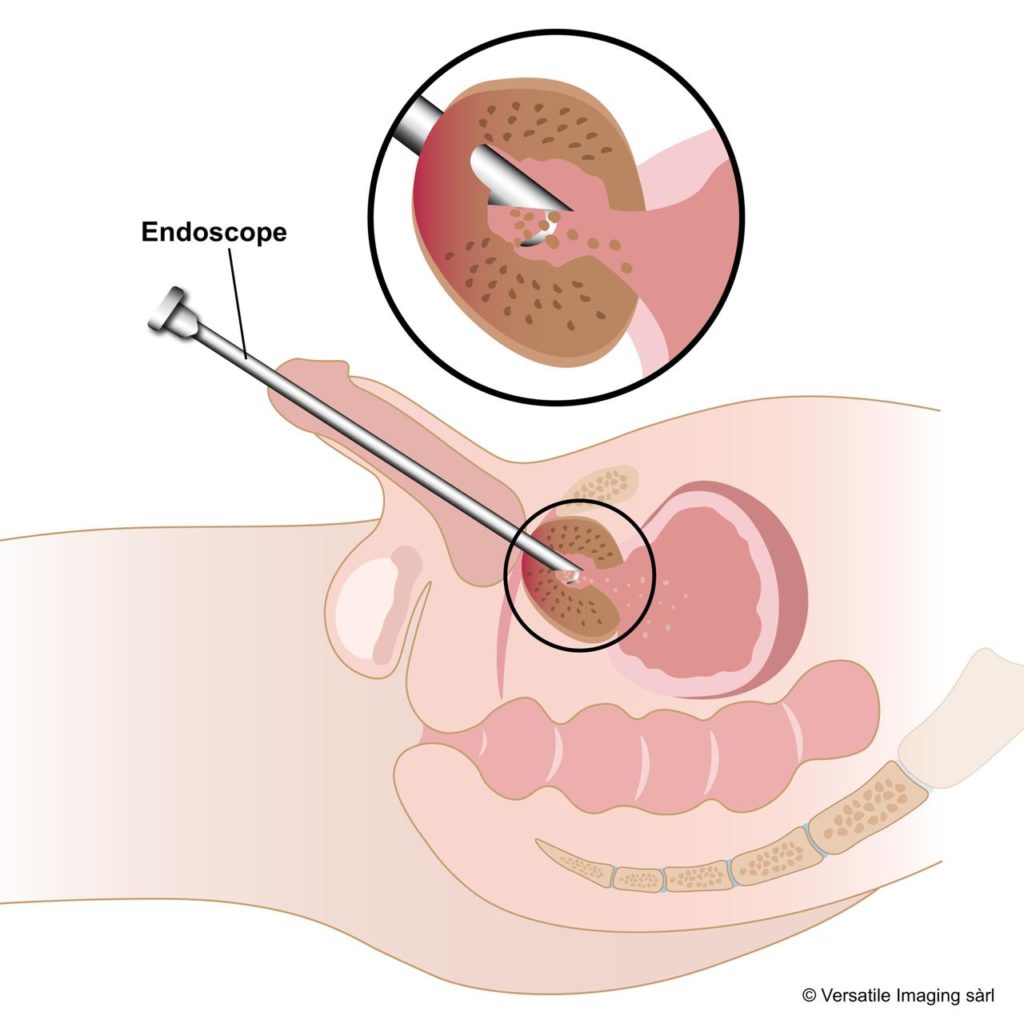
Endoscopic prostate resection treatments (passage through the urethra) (transurethral resection of the prostate or TURP) are generally performed under general anaesthesia during a short hospitalisation, with a post-operative bladder catheter, more rarely as an outpatient under local anaesthesia. It is also the urologist who performs this treatment, which involves cutting away hypertrophied prostate tissue under visual control using a rigid endoscope inserted through the urethra. Continuous irrigation pushes the shavings towards the bladder and these are collected at the end of the procedure. A variant called vaporisation (steam jets, laser, etc.) allows the prostate to be destroyed using the same approach. Post-operative recovery is generally marked by pain lasting several days and an irritative bladder syndrome (weeks to months). These endoscopic treatments are associated with complications such as:
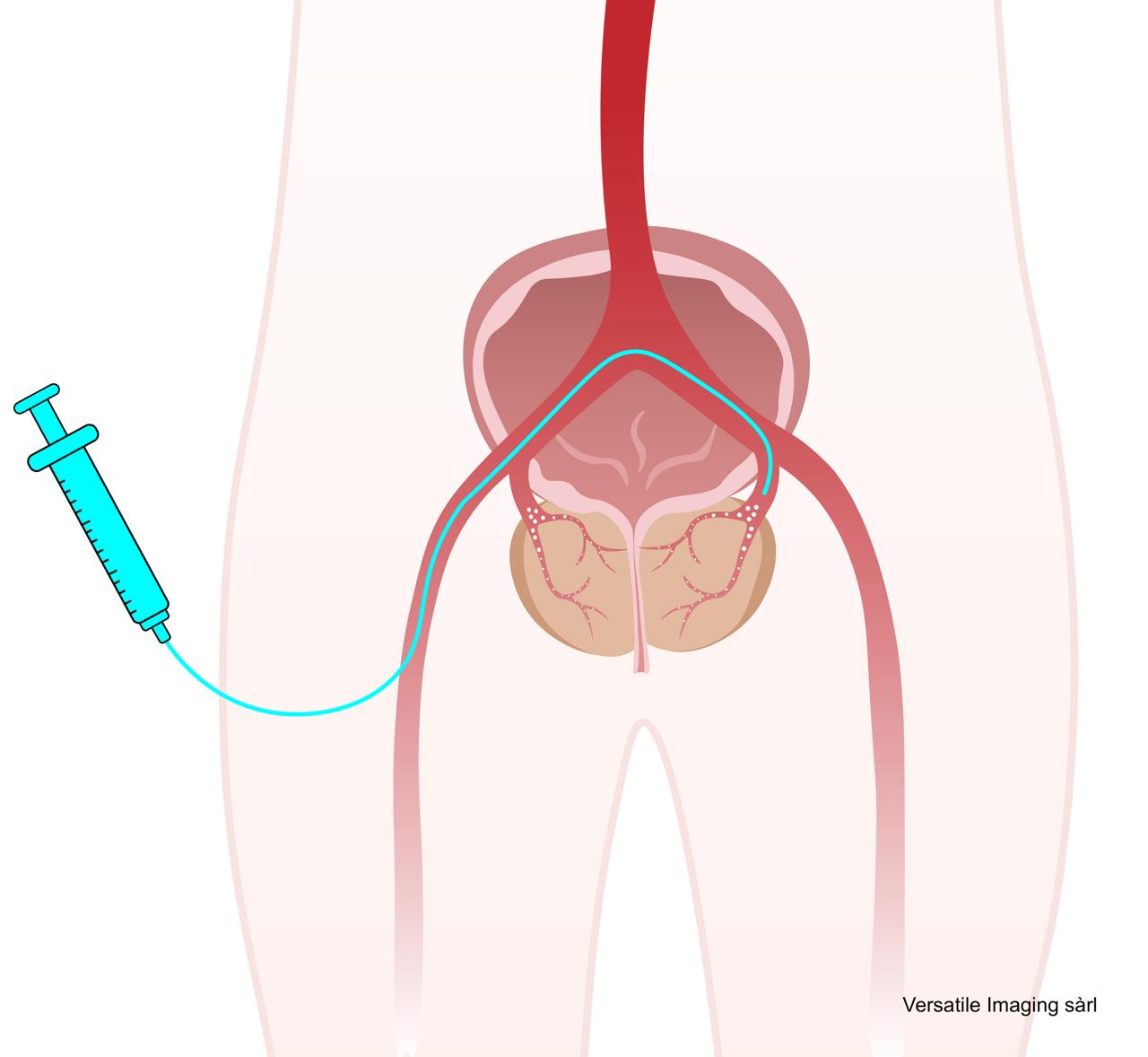
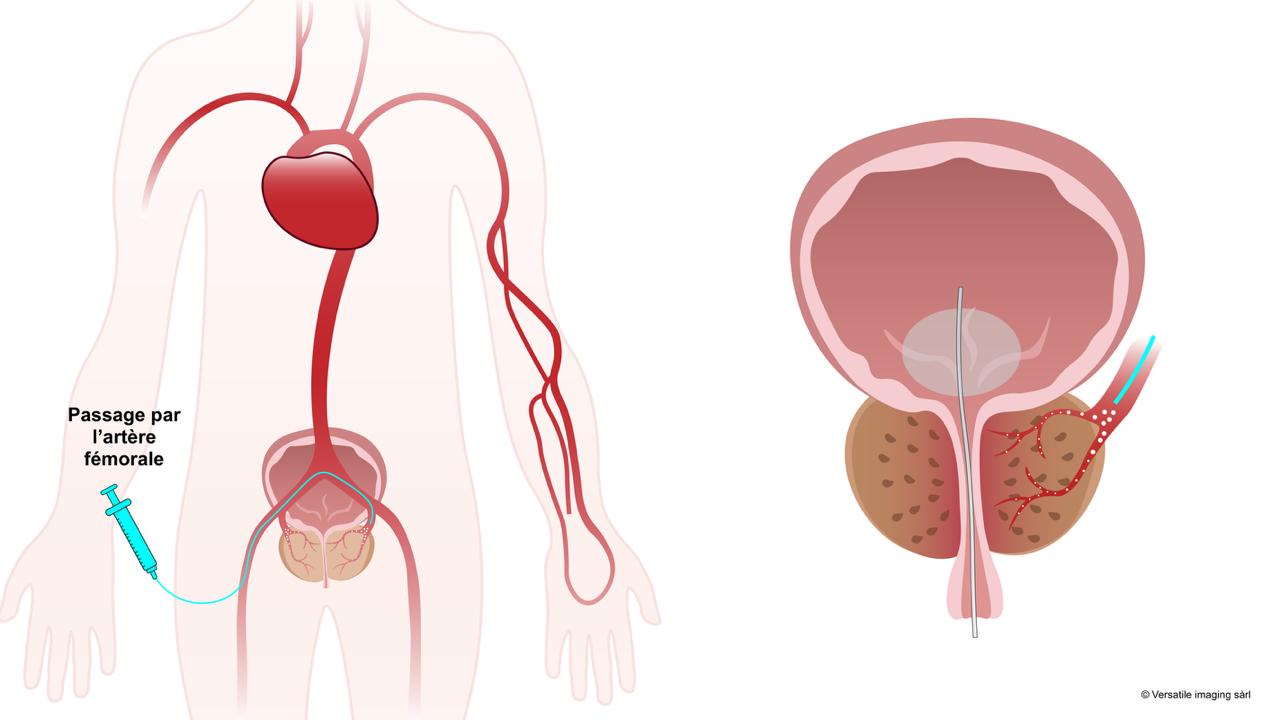
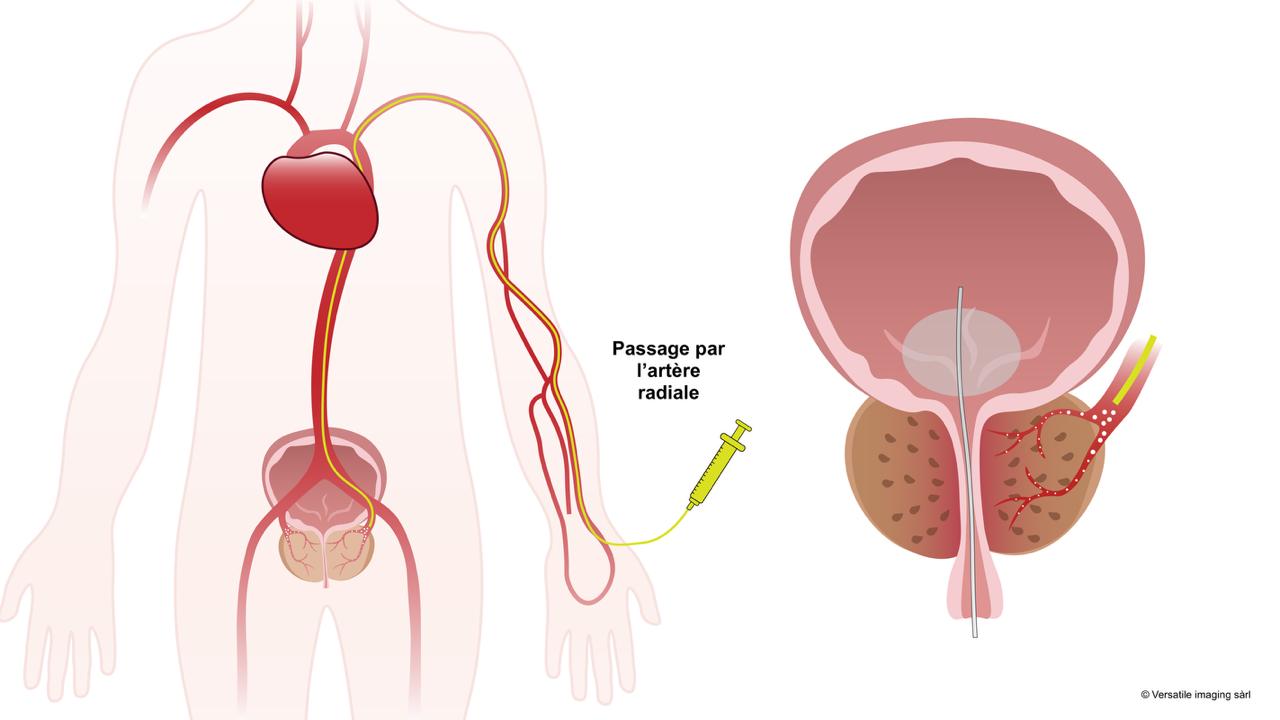
The principle is different from endoscopic urological treatments. Rather than resecting and evacuating the hypertrophied tissue, the aim is to dry it out by depriving it of its blood supply. The prostate then gradually decreases in size. The radiologist enters through the skin into the small arteries that bring blood to the prostate and blocks them on each side. It is a quick procedure (1-3h), performed as an outpatient, painless and covered by basic LAMal insurance.
During your first contact with the interventional radiologist, you will be asked to gather a series of medical data (urology reports, images (CD, USB key, cloud) and prostate MRI report, etc.) that will allow the radiologist to determine if you are a good candidate for this treatment during your pre-interventional consultation. The prostate MRI is particularly important to exclude signs of prostate cancer, which constitutes one of the rare contraindications. Your operator may also ask you to have a CT angiogram (a technique different from MRI) which helps to clarify the particular anatomy of your fine prostatic arteries, facilitating catheterisation during the procedure.
During the pre-interventional consultation, you will be asked to fill in two questionnaires to assess your obstructive urinary symptoms and your erectile sexual function. You can freely download these questionnaires and fill them in before your consultation. A basic blood test will be performed. A urine analysis is sometimes also carried out. A urinary flow meter will serve as a baseline for post-treatment follow-up.
The procedure is performed as an outpatient or during a short hospitalisation. It is carried out by interventional radiologists in an interventional radiology suite, under local anaesthesia. A urinary catheter may be placed.
The operation takes place in a sterile environment similar to an operating theatre. You will be undressed and positioned on the radiology table. Medical staff will set up an IV line, then after disinfecting your groin or wrist one final time, you will be covered with sterile drapes.
The duration of prostatic embolisation varies between 1.5 and 3 hours, depending on the anatomy of the pelvic and prostatic arteries, which can sometimes make access more complex due to significant tortuosities.
Your interventional radiologist will then see you in consultation for follow-up. The two questionnaires you filled in during the pre-interventional consultation will be repeated to assess the benefit on your symptoms. The follow-up schedule is adapted to each individual case (generally at 3-6 months). Often, an MRI examination is repeated to better evaluate the necrosis of the hypertrophied portion of the prostate and its size reduction. Urinary flow meter tests will also be repeated.
| Criteria | TURP / Surgery | Embolisation (PAE) |
|---|---|---|
| Hospitalisation | Yes (several days, urinary catheter) | Outpatient or short hospitalisation |
| Anaesthesia | General or spinal | Local +/- sedation |
| Incision | Endoscopic (urethral) | None (arterial puncture) |
| Retrograde ejaculation | 30–40% (TURP), near-constant (laser) | No |
| Erectile dysfunction | Possible | No |
| Recovery | Several weeks | A few days |
| Bleeding risk | 2% (transfusion) | Very low |
| Retreatment possible | Yes, but higher risk | Yes, straightforward |
Prostatic artery embolisation is a therapy that can now be offered early, as an alternative to medication or surgical/endoscopic treatment.
The objective of the PARTEM study was to evaluate the two-year effects of a minimally invasive approach, prostatic artery embolisation (PAE), compared to medical treatment in patients with a prostatic adenoma greater than 50 g.
The study recruited 90 patients across 10 hospital centres in France, between September 2016 and February 2020. All patients had troublesome urinary symptoms, despite alpha-blocker treatment, and these symptoms were measured by the International Prostatic Symptom Score (IPSS).
Patients were randomly assigned to two groups: 44 received PAE and 43 were treated with a combination of dutasteride (0.5 mg) and tamsulosin (0.4 mg) administered daily.
After 9 months, a significant reduction in symptoms was observed in the PAE group, compared to the combined treatment group, both clinically and statistically. Moreover, notable improvements were observed regarding sexual symptoms in the PAE group. The procedure, performed as day surgery, was accompanied by some minor side effects immediately after the intervention.
A recent 2024 randomised study, called 'P-EASY ADVANCE', examined the efficacy of prostatic artery embolisation (PAE) compared to combined drug therapy of tamsulosin and dutasteride in men suffering from benign prostatic hyperplasia (BPH) who had received no previous treatment. The study was conducted with 39 men divided into two groups, receiving either drug treatment or PAE, with follow-up including urodynamic studies, symptom evaluations (IPSS), and ultrasounds. The results show that both interventions improve urinary symptoms, but PAE offers superior advantages. Patients who underwent PAE observed a more significant reduction in prostate size, a decrease in incomplete emptying symptoms, and a more marked increase in maximum urinary flow rate (Qmax) compared to the medication group. Moreover, PAE led to a notable improvement in participants' quality of life. In contrast, drug treatment was associated with more sexual side effects such as ejaculation disorders, while PAE side effects, such as increased urinary frequency and urination pain, proved to be transient.
These results show that prostatic artery embolisation appears as an effective alternative to drug treatment for men with BPH who have never been treated. This study is the first to compare PAE and combined therapy in treatment-naïve patients, suggesting that PAE could be considered as a first-line option to alleviate urinary symptoms and improve quality of life, with a more favourable side-effect profile than medication.
Even more recently (2024), a scientific study called a meta-analysis compared prostatic artery embolisation to surgical procedures such as transurethral endoscopic prostate resection and simple open prostatectomy for treating benign prostatic hyperplasia. The results show that embolisation is an effective treatment for improving symptoms and urodynamic measures and that it especially offers advantages in reducing complications.

Interventional radiologist
Dr Nicolas Villard is a Swiss physician specialised in interventional radiology. An expert in prostatic artery embolisation, he offers this innovative minimally invasive technique to patients in Western Switzerland.
Drawing on his expertise in interventional radiology and embolisation, he masters the most advanced techniques to ensure optimal results while minimising risks for the patient.
He practises in Lausanne and Geneva, in close collaboration with urologists in the region. Consultations are available in French, English or German.
Clinique Générale Beaulieu
Chemin de Beau-Soleil 20, 1206 Geneva
List of other doctors performing this procedure in Western Switzerland →
For a consultation, contact Dr Villard's office.
Please forward your recent results (urology reports, prostate MRI, blood tests) to the office.
Select a time slot online for a consultation in Geneva or Lausanne.
Note: It is essential to consult your specialist interventional radiologist for personalised information adapted to your health condition.